Q&A with Jen Strohecker: Leading Through Crisis and Closing Cracks in Care
Utah Medicaid Director Jen Strohecker shares insights on managing a cyberattack crisis, building sustainable funding for adult expansion,...
Medicaid agencies use a variety of strategies to oversee providers and managed care plans, and to ensure that Medicaid members meet eligibility requirements.
As of January 2025, Medicaid and CHIP (the Children’s Health Insurance Program) provided health coverage to 78.4 million people, and as of FY 2023, accounted for about $880 billion in total state and federal spending. Because Medicaid is jointly administered by states, territories, and the federal government, Medicaid agencies play a key role in preventing fraud, waste, and abuse in the program. As part of their core operations, Medicaid agencies use a variety of strategies to oversee providers and managed care plans, and to ensure that Medicaid members meet eligibility requirements.
How do Medicaid agencies and the federal government address fraud and abuse?
Unlike waste, fraud and abuse are addressed in federal law and can result in civil, criminal, and administrative penalties. States, territories, and the federal government each play key roles in detecting, investigating, addressing, and preventing fraud and abuse in Medicaid.

States, territories, and the federal government use a range of tools to identify potential fraud and abuse in the Medicaid program. These efforts include data analytics, audit strategies, and stakeholder reporting.
When potential fraud or abuse is identified, Medicaid programs initiate formal investigations in partnership with state, territory, and federal entities.
State, territory, and federal entities may pursue enforcement actions when they find evidence of fraud or abuse. Enforcement tools include a range of options such as recouping funds that have been improperly paid, monetary fines, and, in more serious cases, arrests and criminal convictions. Although fraud cannot be comprehensively measured in Medicaid, providers—rather than Medicaid members—account for the vast majority of fraud-related criminal convictions and monetary recoveries. 
States, territories, and the federal government take numerous steps to prevent fraud and abuse from occurring.
While most Medicaid fraud and abuse is not perpetrated by Medicaid members, ensuring that individuals who are enrolled in the Medicaid program meet eligibility requirements is a core element of program integrity. Medicaid agencies use a variety of strategies, including electronic data checks and regular redeterminations of eligibility, to ensure that individuals enrolled in their programs meet eligibility requirements.
Federal law establishes minimum eligibility requirements for Medicaid. There are many factors that impact Medicaid eligibility, including citizenship, state residency, income, assets (for some coverage groups), and household composition. All states and territories cover certain mandatory eligibility groups, including low-income children, low-income pregnant women, certain parents and caregivers, and individuals receiving Supplemental Security Income, and can choose to cover additional eligibility groups.
How do Medicaid agencies make sure that individuals who are enrolled in the program meet these eligibility requirements? Under federal law, Medicaid agencies are required to check member eligibility when individuals newly apply for Medicaid and during annual renewals. Medicaid members are also required to report when they experience “changes in circumstances,” like changes in income, household composition, or residency, that may affect eligibility status.
Eligibility determinations are conducted by state and territory eligibility workers and by eligibility and enrollment IT systems, which check electronic data sources like the Internal Revenue Service and other social service programs like the Supplemental Nutrition Assistance Program. At application, states and territories check the information provided by applications against tax records, wage data, and other electronic sources to verify accuracy. If the information provided by the applicant is not “reasonably compatible” – or similar enough – to the data provided by these electronic sources, the applicant is asked to provide additional documentation. At renewal, Medicaid agencies are required to check these electronic data sources to see if they can automatically renew the individual’s eligibility before requesting additional documentation. This use of electronic data sources helps improve the accuracy of eligibility determinations, reduces workload for eligibility staff, and reduces reporting burden on Medicaid members.
In addition to these automatic data checks, states and territories use a variety of strategies to ensure that enrolled Medicaid members are eligible for the program. All Medicaid agencies use the federal Public Assistance Reporting Information System (PARIS), which indicates if a Medicaid member may be enrolled in two states simultaneously; this data can often lag by several months, however.
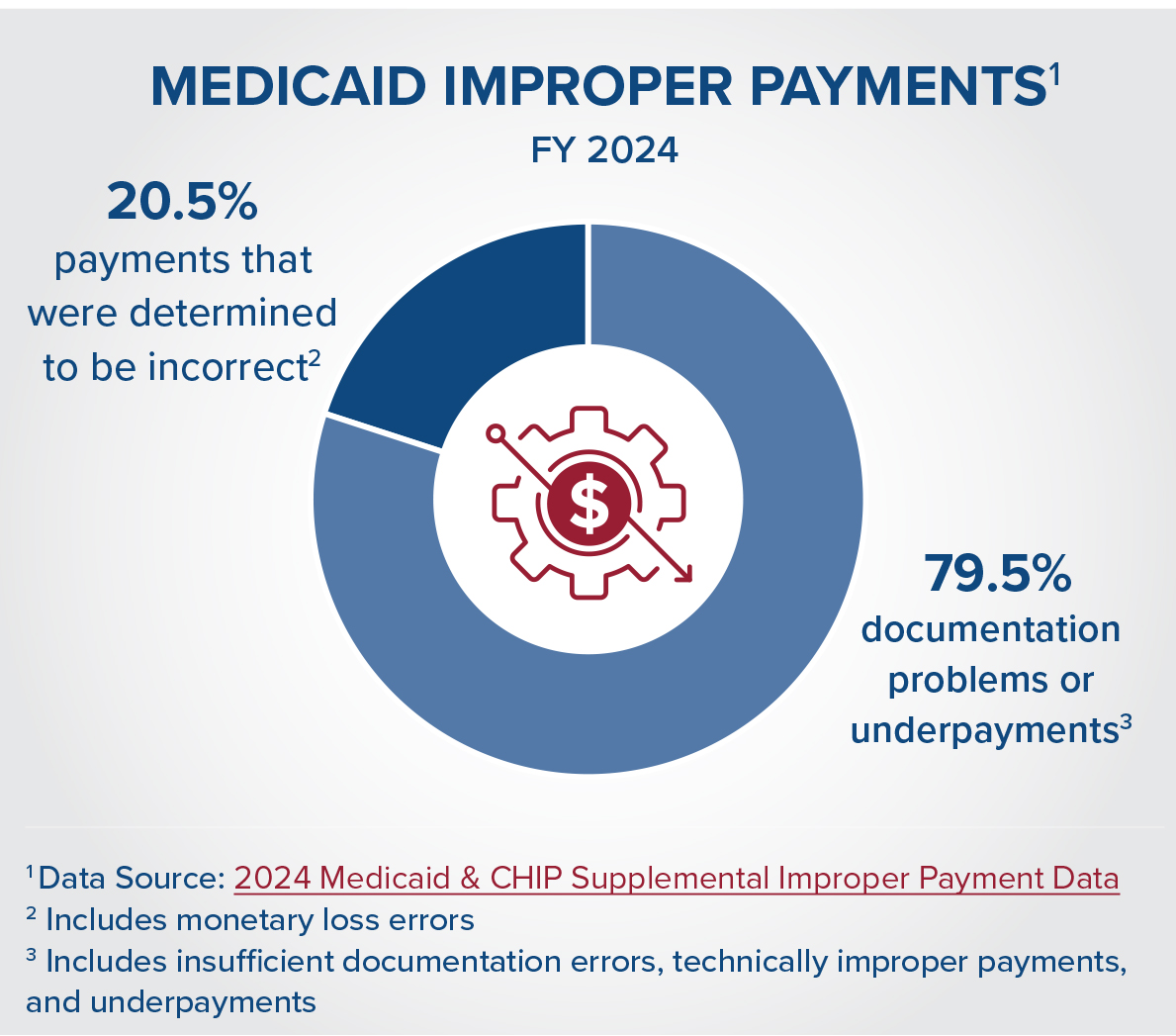
Medicaid agencies and the federal government also regularly audit eligibility systems for errors, including through the Payment Error Rate Methodology (PERM) audit. Although PERM is sometimes pointed to as a measure of fraud in the program, it is important to note that the majority of PERM errors are related to documentation issues, not fraud. For example, in 2024, about 74 percent of improper payments in Medicaid were due to insufficient documentation, meaning that HHS could not determine if the payment was corrector incorrect. Under current law, the Secretary of Health and Human Services (HHS) has the authority to withhold federal Medicaid payments if a state’s improper payment rate exceeds a 3% threshold, or to collaborate with the state on a corrective action plan to reduce improper payments. As part of these corrective action plans, states participate in the Medicaid Eligibility Quality Review (MEQC) program, which supports states in identifying and addressing the root causes of eligibility errors.
Finally, Medicaid agencies use strategies to identify if members have other sources of health care coverage, such Medicare, private insurance, or veterans’ health benefits. Medicaid is generally the “payer of last resort,” meaning that if an individual has more than one coverage source, their other insurer must pay for covered care before Medicaid will cover any remaining services. Medicaid agencies ask members for information about other forms of health coverage at application and renewal, and also use data matches to identify other sources of coverage. If a Medicaid member does have more than one source of health coverage, the Medicaid agency will coordinate with that other payer to ensure that claims are paid in the proper order.
Most Medicaid programs deliver care to members through contracts with private managed care organizations (MCOs). About 75 percent of Medicaid members are enrolled in managed care, under which MCOs receive a defined monthly payment amount for each enrollee, also referred to as capitation. In exchange, MCOs must provide necessary coverage and services for that enrollee. Because MCOs account for the majority of Medicaid spending and care delivery, oversight of MCOs is a top priority for states, territories, and the federal government.
Medicaid agencies use contracts to establish standards for managed care organizations. Under federal law, these contracts must include requirements that plans implement processes to detect and prevent fraud, waste, and abuse. These required processes include establishing compliance officers and committees, training managed care plan leadership and employees, and conducting routine internal audits.
In addition to these program integrity requirements, states and territories use a variety of tools, including ongoing monitoring of network adequacy, quality, and fiscal health, to ensure that managed care plans are following contract requirements and federal regulations. When Medicaid agencies identify issues, they use a variety of strategies to bring managed care plans back into compliance. These range from corrective action plans, which outline steps managed care plans need to take to resolve issues, to liquidated damages and financial penalties. In the most serious cases, Medicaid agencies can suspend payments to managed care plans or disbar plans from participating in the Medicaid program.
Medicaid agencies also use strategies to ensure efficient delivery of care through managed care organizations. These strategies include:
What strategies do Medicaid agencies use to reduce waste?
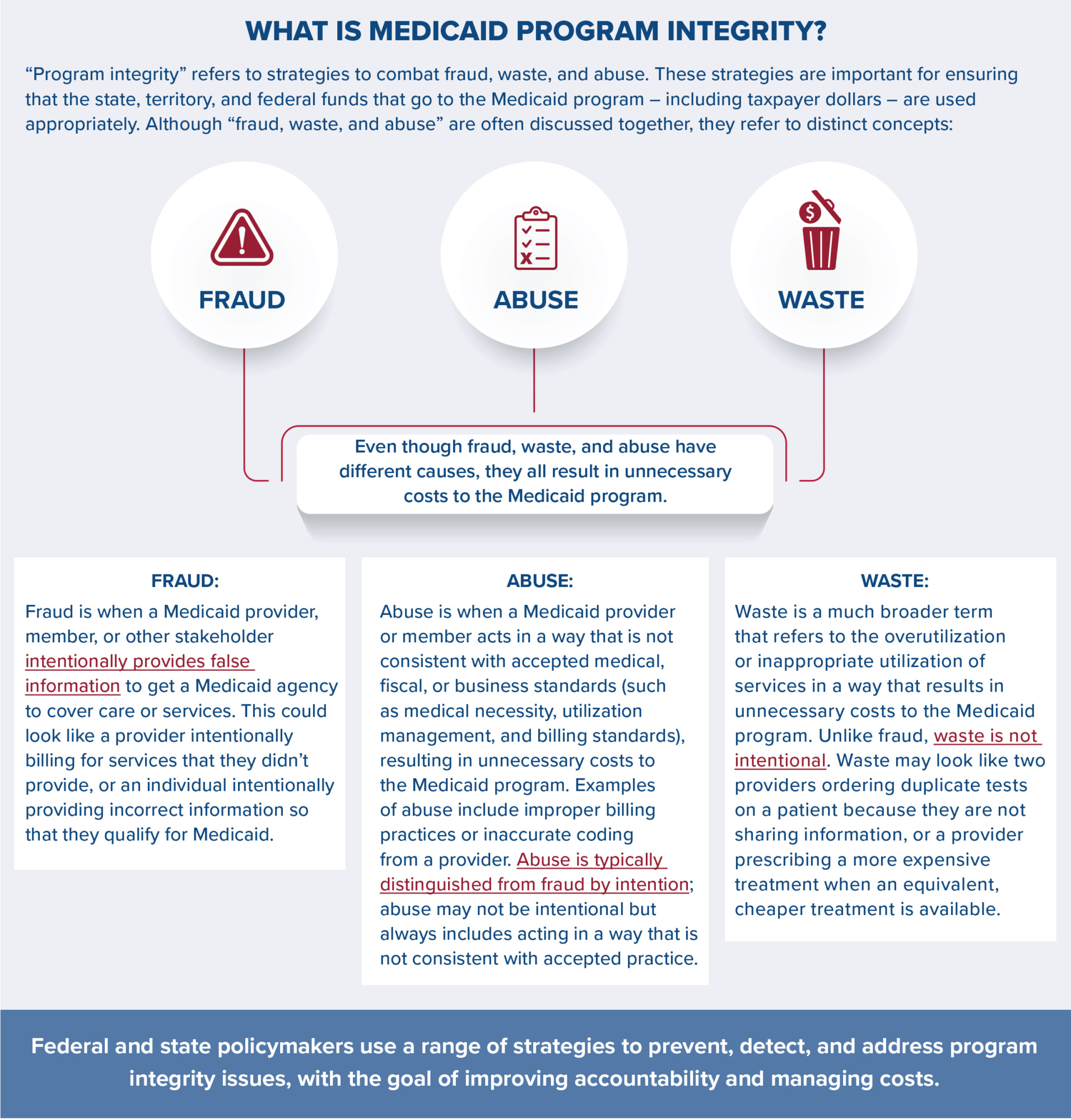
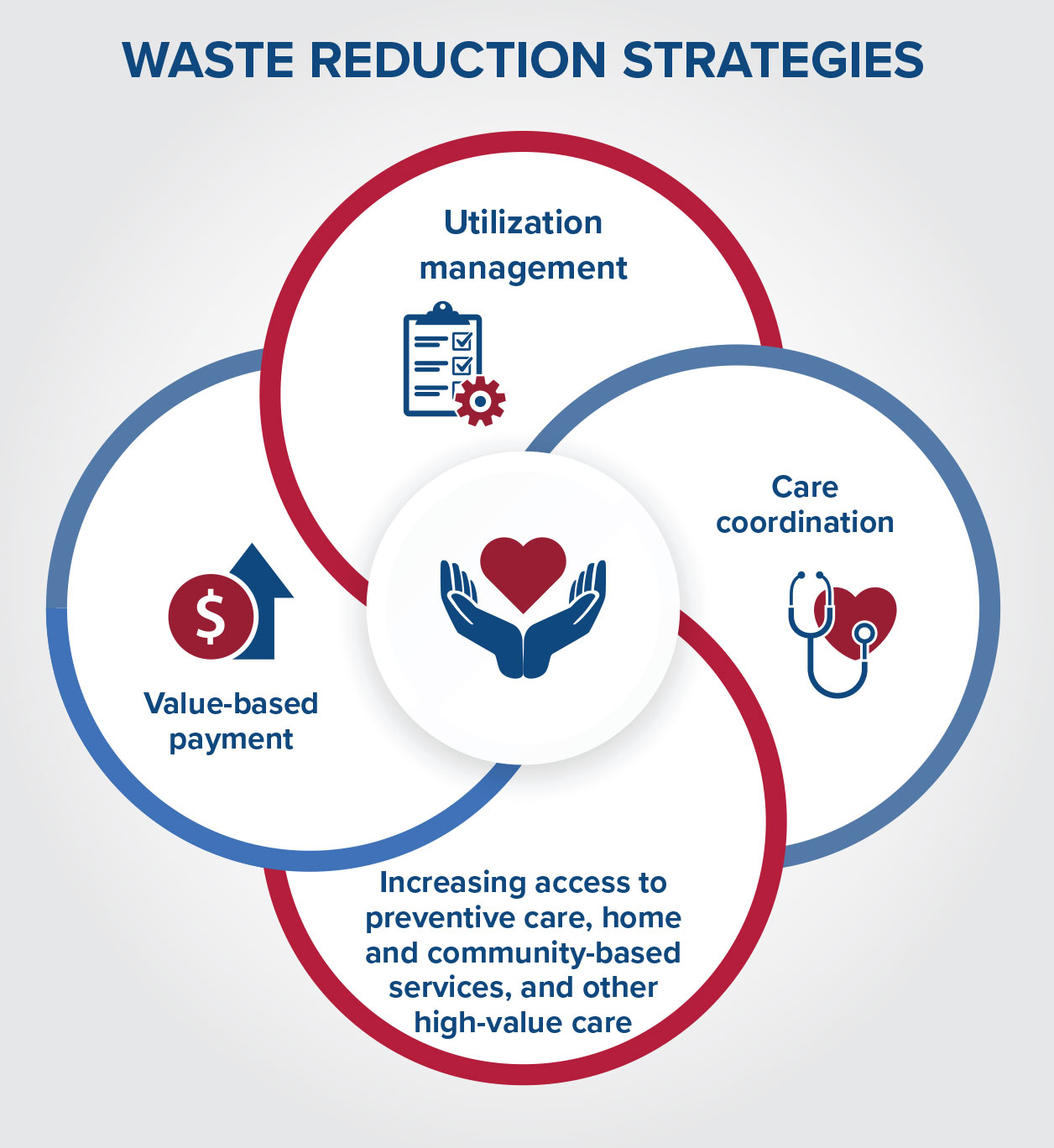
Waste is a much broader concept than fraud and abuse, and refers to duplicative or excessively costly care. Unlike fraud and abuse, which are defined in program integrity regulations and are typically investigated and prosecuted, waste is unintentional. Medicaid agencies and other health care entities are addressing waste through value-based payment, service delivery reforms, and care management strategies that aim to improve the efficiency of services and ensure they are appropriate.
Common strategies to reduce waste in the Medicaid system include:
Fraud, waste, and abuse are distinct concepts, but all result in unnecessary costs to the Medicaid program. States, territories, and the federal government use a range of strategies to address fraud and abuse and to reduce waste. These programintegrity practices are crucial for ensuring that state and federal funds are used appropriately and efficiently.
Drop us your email and we’ll keep you up-to-date on Medicaid issues.